A 60 yr old male
Chief complaints :










A 60 yr old male came to OPD with chief complaints of altered behaviour and vomiting
HOPI :
Patient was apparently asymptomatic 12 years back , then he developed dizziness and weakness , on examination in local hospital he was diagnosed with diabetes , then onwards he was on OHAs taking one tablet a day , this continued for 6 years , then due to uncontrolled blood sugar levels he had to increase his dose to twice a day , then from past 3 years he's on Regular insulin injection (15 IU in morning and 10 IU units in evening ) , 4 months back while he was driving accidentally he has burnt his right foot due to silencer ( exhaust ) , which got infected , that led to amputation of his 3 right lateral toes , after on general check up he was informed that his blood sugars are in control and was asked to take OHAs .
3 days back he attended a function where he had consumed alcohol , had non veg , he skipped his medication on that evening , then he reported to have altered behaviour and vomiting of few episodes which is non bilious , non projectile , non foul smelling , content - food in the first episode ,later on it was watery .
Past history :
K/c/ o DM type 2 since 12 years
HTN
Not a known case of bronchial asthma , tuberculosis , epilepsy , Thyroid abnormalities .
Treatment history :
Personal history :
Diet: mixed
Appetite - normal
Sleep - adequate
B/B movements - regular
Addictions - Alcoholic since age of 15 years( whisky )
No allergies
Family history :
No significant family history
On examination : patient is drowsy , incoherent speech .
GCS score : E4, V3, M6
Moderately built and nourished.
Pallor , icterus , cyanosis , clubbing , lymphadenopathy , edema - absent


Systemic examination :
Pulse - 76 bpm
BP 220/110 mmhg
Spo2 - 98
Resp system : BAE present , normal vesicular breath sounds heard
CVS : S1 , S2 heard , no murmurs detected
CNS examination : No focal neurological dafects present
P/A : soft , non tender , no organo megaly present
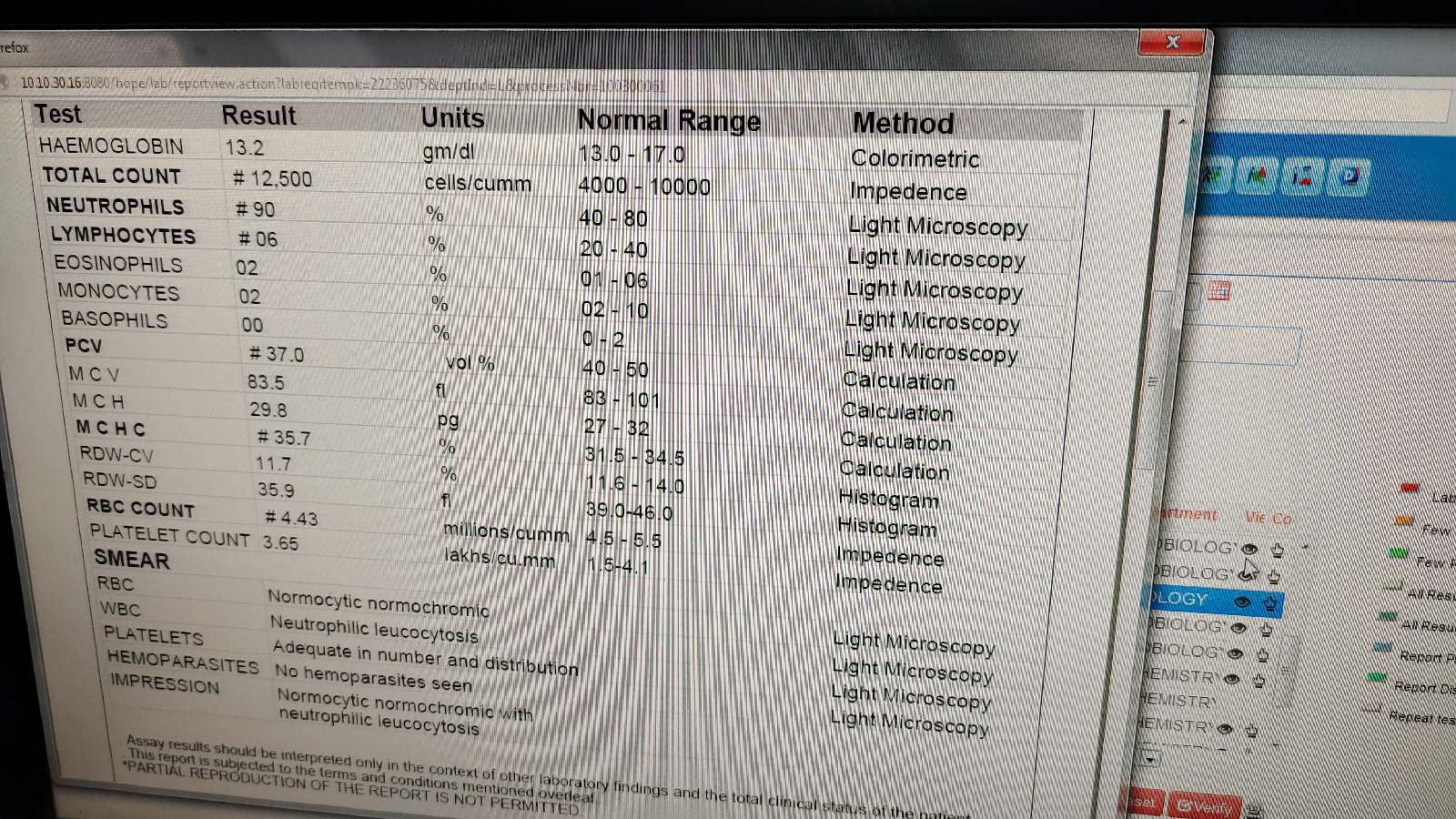
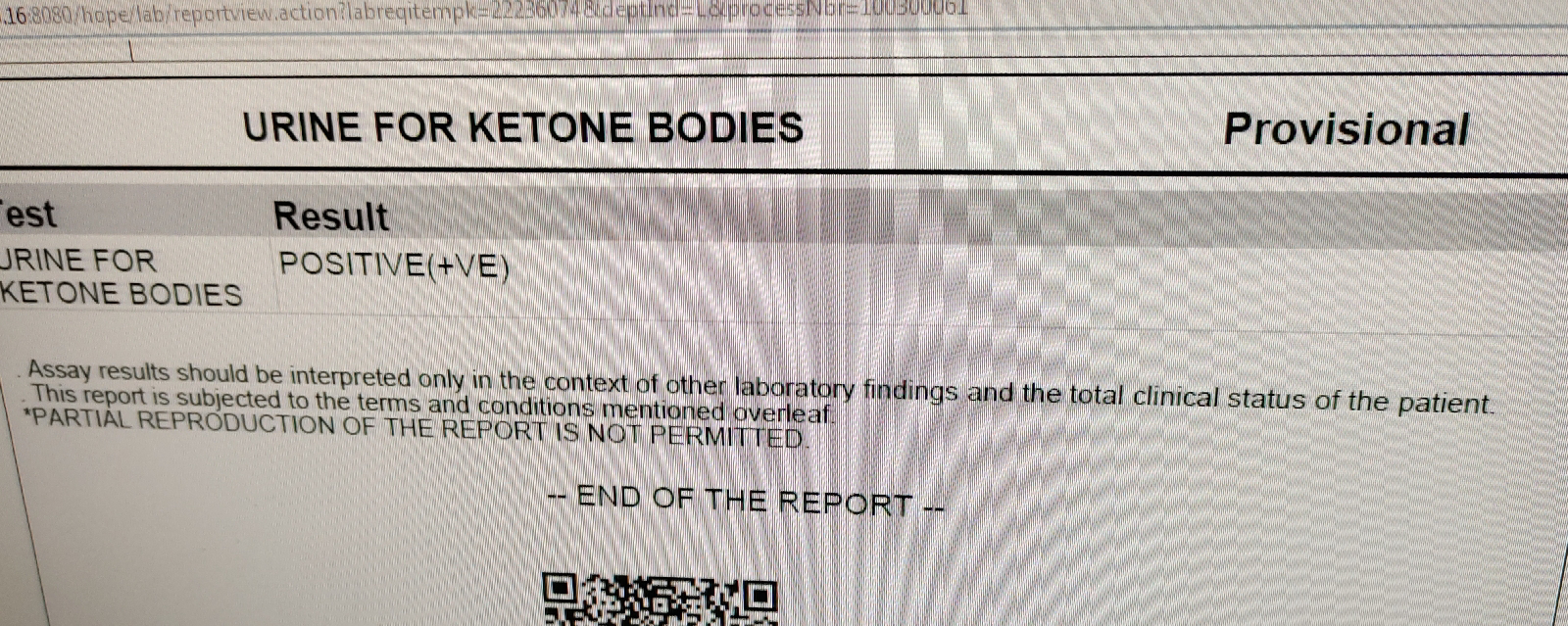
Investigations :


Provisional diagnosis : DKA
Treatment :
Iv - NS @ 125 ml / hr
INJ- THIAMINE 2 ampules in 100ml NS I.v
Tab- NICARDIA
BP/PR/temp - monitor 4th hrly
INJ - lorazepam
INJ - haloperidol 5 mg I.M



Comments
Post a Comment